

Background
Diffuse Large B-Cell Lymphoma (DLBCL) is the most common subtype of non-Hodgkin lymphoma (NHL), accounting for approximately 22% of newly diagnosed non-Hodgkin's lymphoma per year in the United States. Combination chemoimmunotherapy with or without radiation therapy is recommended for the upfront treatment of DLBCL (Yang Liu, AJH,2019). A minority of patients undergo surgery prior to the initiation of systemic therapy for symptom relief or treatment of complications related to the disease. There are concerns on the delay in initiation of systemic therapy when surgery is performed and the potential impact on long term survival in this aggressive chemosensitive disease. We aimed to explore the characteristics of patients undergoing surgery prior to systemic therapy (sxfirst), the predictors for sxfirst and the survival outcomes.
Methods
We queried the National Cancer Database for patients with DLBCL (ICD-0-3 code 9680) diagnosed from 2006-2015. Inclusion criteria were patients that received systemic therapy as first-line course of treatment and excluded patients with incomplete or missing data for disease stage, treatment characteristics and follow-up. We also excluded patients who underwent biopsy procedures for diagnosis and local procedures such as tumor destruction or ablation. Subgroup analysis of patients that received sxfirst was performed. Time-to-initial therapy (TTI) was defined as time in days (d) from diagnosis to systemic therapy. Survival was measured in terms of months (m) from the day of diagnosis. Stepwise multivariate logistic regression analysis for predictors of sxfirst and propensity score adjusted survival analysis was performed.
Results
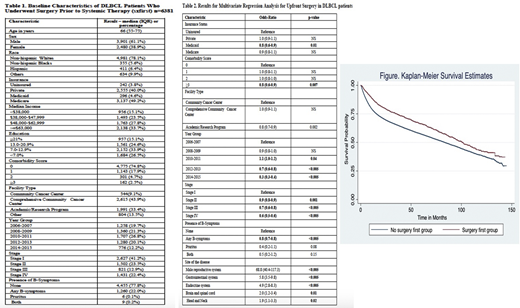
Of 208,748 patients with DLBCL, 138,096 patients met the inclusion criteria of whom 6,381 (4.6%) were sxfirst. The characteristics of sxfirst are summarized in Table 1. Median age was 66 (interquartile range IQR 55-75) years and 61.1% were males. Majority were non-Hispanic whites, had private or medicare insurance, had comorbidity score of 0 and stage I disease. Most patients were treated in comprehensive community cancer centers. The top 5 extra-nodal disease sites were gastrointestinal (26.2%), male reproductive system (16.4%), brain and spinal cord (6.4%), endocrine system (4.1%) and head and neck (3.0%). The median follow up was 47.6 (IQR 14.0-78.9) months. The predictors for sxfirst are described in Table 2. The following disease sites were associated with higher likelihood of sxfirst: male reproductive system (p-value<0.005), gastrointestinal system (p-value<0.005), endocrine system (p-value<0.005), brain and spinal cord (p-value=0.01) and head and neck (p-value=0.02) while the following factors were associated with lower likelihood of sxfirst - medicaid insurance (p-value=0.01), comorbidity score >=3 (p-value 0.007), more recent year of diagnosis, advanced stages of disease and presence of B-symptoms. The TTI for systemic therapy was delayed in sxfirst group - 34 (IQR 22-51) days vs. 21 (IQR 11-35) days, p-value<0.005. The 5-year overall survival for the sxfirst group was 64% (95% CI 62-65%) vs. 57% (95% CI 56-57%)- HR 0.75 (95% CI 0.71 - 0.81). The factors associated with increased mortality were advanced age, higher comorbidity score, lower educational status, advanced clinical stage of the disease, presence of B-symptoms , disease primarily located in the bone, brain and spinal cord.
Conclusion
The findings of the present study are twofold. First, the present study describes the characteristics and predictors of sxfirst among DLBCL patients. Second, if surgery is absolutely necessary prior to systemically treating DLBCL, the study suggests that the delay does not seem to impact long term survival of these patients and is similar to the 5-year overall survival (64%) reported for DLBCL when all stages and treatment strategies are combined (seer.cancer.gov/statfacts/dlbcl). While there are unmeasured confounding factors as a result of the absence of adequate prognostic markers and treatment characteristics in the database, it is possible that surgery truly doesn't impact the survival outcomes significantly. Further evaluation of this practical question is warranted in large scale prospective studies.
Khan:Abbvie: Honoraria; Genentech: Honoraria; AstraZeneca: Honoraria; Takeda: Honoraria; Celgene: Honoraria; Karyopharm: Honoraria; Beigene: Honoraria; Seattle Genetics: Honoraria. Fazal:Stemline: Consultancy, Speakers Bureau; Jazz Pharma: Consultancy, Speakers Bureau; Jansen: Speakers Bureau; Karyopham: Speakers Bureau; Incyte Corporation: Consultancy, Honoraria, Speakers Bureau; Takeda: Consultancy, Speakers Bureau; Agios: Consultancy, Speakers Bureau; Glaxosmith Kline: Consultancy, Speakers Bureau; Gilead/Kite: Consultancy, Speakers Bureau; Novartis: Consultancy, Speakers Bureau; Celgene: Speakers Bureau; Amgen: Consultancy, Speakers Bureau; BMS: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Speakers Bureau.

